Practicing Affective Granularity: Tools for Daily Emotional Precision
Struggling with emotional rigidity, perfectionism, or cycles of despair that never seem to shift? Traditional coping strategies often skim the surface, offering temporary relief without addressing the deeper architecture of our emotional lives. The Core Emotion Framework (CEF) introduces a groundbreaking, high‑resolution model of affective granularity—the ability to distinguish, compose, and regulate emotions with precision. By mapping all complex feelings onto ten Core Dimensions, CEF empowers individuals to move beyond vague self‑help buzzwords and into a structured practice of emotional mastery. This article explores the compositional mechanics of affective granularity, showing how vulnerability can be transformed into resilience, and how psychological flexibility can be cultivated through a deeper understanding of emotional structure
The Science of Emotional Composition: Building Blocks of Resilient Self‑Mastery
Are you tired of generalized coping strategies that fail to address the root of your emotional struggles? The Core Emotion Framework (CEF) provides the high-resolution architectural map needed to dismantle the cycles of emotional rigidity and unlock psychological flexibility. This deep-dive analysis demonstrates how all complex feelings—from despair to perfectionism—are synthesized from ten fundamental Core Dimensions. By mastering the compositional mechanics of these dimensions, individuals gain true emotional granularity, transforming vulnerability into resilient self-mastery and paving a transformative path toward sustainable mental well-being.











The Compositional Mechanics of Affective Granularity: A High-Resolution Expansion of the Core Emotion Framework (CEF) for Treating Psychological Rigidity

I. Beyond Buzzwords: Unlocking the Transformative Power of Affective Granularity
The field of psychology is currently experiencing a critical transition away from foundational categorical models of emotion toward more nuanced dimensional approaches. This shift acknowledges the limitations of viewing complex psychopathology through the lens of strictly defined basic emotions, recognizing instead that all affective states emerge from shared, overlapping neurophysiological systems. While dimensional models offer quantitative improvements in understanding human affect, they frequently lack the structural specificity required for targeted clinical intervention, often failing to clarify the developmental genesis or specific mechanism of life dysfunction in psychiatric traits.
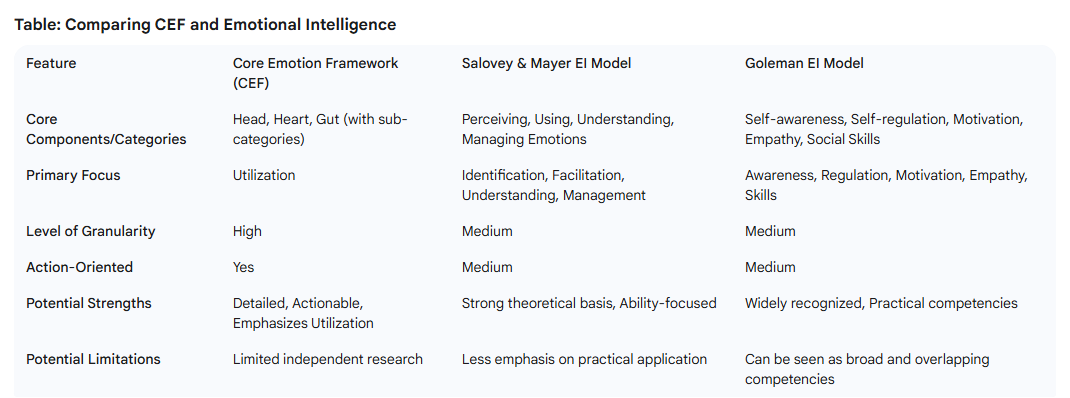
The Core Emotion Framework (CEF) provides a necessary structural-constructivist solution to this problem. CEF posits that the entire spectrum of human emotional experiences and character traits are synthesized from a finite, universal set of ten fundamental psychological capacities termed "Core Emotions".1 These elements are organized within a tripartite architecture—the Cognitive Center (Head), the Affective Center (Heart), and the Conative Center (Gut)—which assigns explicit psychological functions to each dimension, transforming abstract dimensional space into a specific, actionable blueprint for emotional experience.1 Crucially, CEF defines complex emotional states, such as fear and anger, not as innate basic emotions, but as "composite states," resulting from the dynamic interplay and aggregation of these underlying core emotional ingredients.4
A central dialectic in mental health research concerns the ability of individuals to perceive and articulate their emotional experiences precisely. This skill, known as affective granularity or emotion differentiation, is strongly associated with positive mental health outcomes. While traditional studies suggest that repeated experience sampling can facilitate an increase in granularity, they often fall short of explaining the operative mechanism underlying this differentiation.5 The CEF addresses this gap directly by operationalizing granularity not as a passive reporting measure, but as an active, compositional competency. The ability to achieve granularity is thus defined by the capacity to accurately identify, differentiate, and intentionally cycle through the ten specific Core Emotions using the framework’s methodology, Adaptive Emotional Cycling (AEC).4
Conversely, psychological dysfunction within the CEF is defined as emotional rigidity: a pathological fusion of these core elements driven by an insistent, limited mode of being. This rigidity is a systemic failure, representing the breakdown of the essential dynamic balance between the primal core capacities of Agency (Assertive Drive, Strategic Order) and Yielding (Receptive Manifestation, Appreciative Resonance). The structural organization of the Core Emotions makes it apparent that treating rigidity requires precision "detangling"—locating and resolving the specific fusion point—rather than relying on generalized flexibility training alone. Health and flourishing are attained through mastering this dynamic balance, achieved via cultivating emotional flexibility.1
II. The Inner Blueprint: Deconstructing Complex States into 10 Core Capacities
The Tripartite Structure and the Ten Primal Capacities
The Core Emotion Framework’s 10 Core Emotions function as the elemental building blocks of the inner world and are organized across three functional centers of the psyche1:
- The Cognitive Center (Head): This center governs perception, conceptualization, analysis, and ultimate choice. It houses Inquisitive Sensing (the capacity for raw, non-conceptual perception and curiosity); Calculating (the capacity for logical evaluation and consistency checking, crucial for clarity); and Deciding (the capacity to synthesize inputs into an actionable conviction).
-
The Affective Center (Heart): This center manages relational dynamics, value judgments, and social esteem. It includes Expansive Openness (the engine of inclusion, generosity, and empathy); Definitive Constriction (the capacity to define, limit, and critique, establishing necessary boundaries); and Harmonious Achievement (the capacity to perform and manifest balance in the pursuit of success and dignity).
- The Conative Center (Gut): Conceptualized as the seat of action and motivation, this center governs execution and drive. It contains Strategic Order (prioritizing, organizing, and defending); Appreciative Resonance (experiencing enjoyment, gratitude, and positive reinforcement); Assertive Drive (the foundational power of agency, akin to the appetitive SEEKING motivational system); and Receptive Manifestation (the foundational power of yielding, acceptance, and surrender).1
The Calculus of Composite States and Diagnostic Precision
The model's strength lies in defining complex affective experiences through a high-resolution calculus of these core components. For instance, the composite state "Fear" is structurally defined as an aggregation of Sensing, Arranging (manage), Accepting (surrender), and Constricting (exactness).4
This compositional definition allows for clinical differentiation: the fear experienced as disorganization during a panic attack (high Sensing, low Strategic Order) is structurally distinct from the fear experienced as hyper-vigilance during high-stakes preparation (controlled Sensing, high Strategic Order).
Applying this compositional clarity to complex, treatment-resistant mood states, such as despair, reveals specific mechanistic targets. Despair, which is fundamentally driven by hopelessness8, can be modeled in CEF as a severe functional deficit in the Conative Center: overwhelming, passive Receptive Manifestation (surrender without agency), coupled with a profound deficiency in Assertive Drive (lack of motivation/push), and a failure of Decisive Knowing (inability to formulate future goals).1 By decomposing despair into these specific core deficiencies, the intervention shifts dramatically, moving from the abstract goal of "treating despair" to the precise, structural target of "activating Assertive Drive." This high-resolution understanding provides an explicit, harnessable power that generalized coping strategies often overlook.8
The framework also provides a powerful diagnostic compass through its assertion of a functional hierarchy. Healthy psychological functioning is posited to follow a top-down sequence: a situation is first perceived (Cognitive Center), its significance is assigned (Affective Center), and an appropriate action is formulated (Conative Center).1 Psychological dysfunction is defined as a "short circuit" in this sequence. This structure allows clinicians to move beyond mere symptom clustering and precisely locate the structural point of failure. If a patient exhibits chronic volitional inertia (a Conative Center failure), assessment can trace the blockage back: was the Cognitive Center stuck in a pathological loop of Structural Analysis (rumination), or did the Affective Center impose excessive Definitive Constriction (self-judgment) that inhibited the energy transfer necessary for action?
III. The Rigidity Trap: Mapping Maladaptive Fusions That Cause Psychological Inertia
Emotional rigidity, the core psychological driver of distress, results from the obstinate inability to yield or change mental thought patterns.1 The temporal manifestation of this rigidity is often perseverative thinking, a maladaptive form of applying cognitive control over time that maintains stress representation and mediates psychological distress.11 The CEF provides a blueprint for understanding this rigidity as the pathological fusion and functional fixedness of Core Emotions.
Case Study A: Analyzing Maladaptive Perfectionism (OCPD)
Obsessive-Compulsive Personality Disorder (OCPD), frequently characterized by an overwhelming preoccupation with perfectionism, organization, and control, is underpinned by rigid beliefs and difficulty relaxing or delegating.12 This condition, often termed "maladaptive perfectionism," can be structurally analyzed in the CEF as a severe, chronic over-reliance on a specific cluster of the 10 Core Emotions—the "Order Tetrad".1
This pathological fusion involves:
- Hyper-Structural Analysis (Calculating): An excessive, persistent focus on rules, consistency, and clarity, causing the individual to get stuck in details and routines.3
- Excessive Definitive Constriction (Constricting): Used rigidly to establish impossibly high standards and drive critical self-evaluation.2
- Over-Strategic Order (Arranging): The pervasive need for control, planning, and defending the system's strict boundaries.12
This rigidity is sustained by the suppression of their complementary Core Emotions, notably Expansive Openness (necessary for flexibility), Receptive Manifestation (necessary for letting go), and Appreciative Resonance (necessary for enjoyment and gratitude).1 The resulting emotional toll, characterized by chronic guilt, anxiety, and burnout13, is the structural failure of the Conative Center, where high Strategic Order fails to be balanced by the necessary rest and positive reinforcement provided by Receptive Manifestation and Appreciative Resonance.4
Case Study B: Affective Inertia and Chronic Rumination
Chronic rumination, characterized by repetitive dwelling on negative feelings and their causes, maintains depression and anxiety by reinforcing negative cognitive and memory biases and inhibiting productive problem-solving.14 Ruminative inertia describes this pattern when it becomes resistant to change .
In the CEF structure, rumination represents a functional short-circuit known as the "Head Loop." The Core Emotion Structural Analysis becomes pathologically perseverative11, running perpetual calculations and dwelling on past events14, but critically failing to transfer this energy to the executive function of Decisive Knowing or the motivational impetus of the Conative Center.1
Furthermore, clinical research indicates that negative rumination bias is significantly more pronounced in the melancholic subgroup of depression compared to the anxious subgroup . This difference suggests a distinct structural failure. While anxious rumination may involve a high-energy loop driven by hyper-vigilant Sensing combined with Calculating future threats, melancholic rigidity can be modeled as a low-energy Calculating loop that has lost access to Assertive Drive (Boosting), the emotional energy parallel to the SEEKING system.1 The failure is fundamentally one of volitional inertia, where the Cognitive Center operates without the capacity for Conative action. This understanding indicates that treatment for melancholic rigidity must prioritize the activation of the Conative Center (Boosting and Arranging) over mere cognitive restructuring of the thought content.
Case Study C: Experiential Avoidance and Trauma Paralysis
Experiential avoidance, defined as the unwillingness to engage with aversive internal experiences (sensations, emotions, thoughts, memories) through the use of avoidance strategies and behavioral inhibition , is a central mechanism underlying numerous psychopathologies, including Complex Post-Traumatic Stress Disorder (C-PTSD).
In CEF terms, experiential avoidance is the strategic suppression of Inquisitive Sensing—the capacity for raw, non-conceptual perception of internal cues—combined with the defensive over-activation of Definitive Constriction to impose rigid internal boundaries against raw emotional data.1 This structural pattern prevents the necessary information processing from occurring. Trauma-linked paralysis or heightened emotional impulsivity16 results from the functional collapse of the Conative Center, where the individual is unable to sustainably activate Assertive Drive or maintain Strategic Order. By blocking the primal power of Sensing, the individual creates an affective black box that prevents functional processing and adaptive movement through the other centers.1
The concept of rigidity, in this context, is equivalent to the phenomenon of functional fixedness7, where a Core Emotion is used only for a limited, familiar, and often maladaptive purpose. The failure is not the existence of the emotion itself (which is viewed as a power to be harnessed1), but the inability to conceive new, utilitarian functions for that Core Emotion. The therapeutic mandate therefore becomes one of shifting the functional context of the stuck element—for example, teaching the client to use Definitive Constriction to enforce healthy boundaries, rather than solely for critical self-judgment or defensive exclusion.
IV. Precision Interventions: The Adaptive Emotional Cycling (AEC) Protocol for Freedom
The therapeutic utility of the CEF is realized through the operational application of emotional flexibility, defined as the speed, range, and coherence of navigating the 10 Core Emotions using the Adaptive Emotional Cycling (AEC) methodology.1 AEC is specifically designed to interrupt the automaticity of psychological rigidity.
Precision Detangling via Complementation
AEC protocols involve the intentional navigation through different emotional states using specific energetic movements (cycling points).4 The core principle of "detangling" a pathological fusion requires the targeted activation of the complementary (diametric) Core Emotion to the one that is pathologically dominant. For example, severe rigidity driven by Definitive Constriction must be balanced by the intentional activation of Expansive Openness.1
Crucially, psychological distress is frequently maintained by maladaptive proactive cognitive control, which drives perseverative thinking.11 AEC introduces a structured, reactive override mechanism designed to interrupt this automatic failure. By forcing a shift away from the stuck center (e.g., the ruminative Head) to an active, volitional center (the Conative Gut), AEC functions as a targeted reset switch, treating the mechanism of perseverative thinking rather than simply debating its content.4
The following protocols illustrate how AEC systematically addresses the identified fusion states by leveraging complementary Core Emotions:
For Maladaptive Perfectionism (OCPD), driven by rigid Definitive Constriction, the necessary complementary activation includes Expansive Openness (Heart) and Appreciative Resonance (Gut).1 The prescribed AEC protocol, termed The Heart Swing, involves cycling between Constricting <-> Expanding, anchored by Appreciating.4 This movement reduces critical self-focus, fosters spontaneity, and provides internal positive reinforcement, thereby disrupting the chronic self-judgment and increasing granularity.
For Ruminative Inertia (Head Loop), rooted in stuck Structural Analysis and deficient Decisive Knowing, the necessary activation is Assertive Drive (Gut) and renewed Decisive Knowing (Head).1 The prescribed AEC protocol is The Decision Thrust: Calculating -> Deciding -> Boosting (Conative Action).4 This breaks cognitive perseveration by transferring stagnant mental energy into immediate volitional movement, thereby activating the SEEKING system parallel of Assertive Drive.2
For Experiential Avoidance (Trauma), characterized by defensive Constriction and suppression of input, the necessary complementation involves Inquisitive Sensing (Head) and Receptive Manifestation (Gut).1 The prescribed AEC protocol, The Grounding Spiral, cycles through Sensing -> Accepting -> Constricting (for controlled safety).4 This practice increases interoceptive awareness without overwhelm and cultivates a safe capacity for yielding and presence.
The Strength-Bridge Mechanism and Appreciative Resonance
The CEF approach naturally integrates strengths-based intervention principles.18 Since Core Emotions are fundamental powers1, chronic rigidity (e.g., in OCPD) demonstrates an underlying, powerful capacity in specific areas, such as robust Strategic Order or strong Structural Analysis.13 Instead of attempting to dismantle this rigid capacity, the clinician can validate and use this strong Core Emotion as a Bridge Mechanism.18 For example, a client’s strength in Strategic Order (Arranging) is leveraged to strategically schedule or order the activation of the missing component, such as Receptive Manifestation (Accepting), thereby forcing the necessary flexibility through the validated power of their existing structure.18
A critical component often overlooked in rigidity models is the specific role of Appreciative Resonance. In high-effort, rigid profiles like OCPD, the failure to activate Appreciative Resonance ensures the cycle of chronic, unrewarded effort continues, resulting in burnout.13 As a Core Emotion in the Conative Center, Appreciating provides essential reinforcement and satisfaction.4 Its deficiency means the psychological system never registers that an "Accomplishment"2 has been successfully completed, driving continued, unceasing effort. Therefore, AEC protocols for burnout and rigidity must intentionally cycle through Appreciative Resonance to successfully reset the internal reward mechanism.
CEF as a Mechanistic Overlay for Third-Wave Therapies
CEF provides the structural language needed to translate the abstract concepts found in third-wave psychotherapies, such as Dialectical Behavior Therapy (DBT) and Acceptance and Commitment Therapy (ACT). DBT emphasizes the dialectic of acceptance and change , while ACT focuses on psychological flexibility and values-driven action.10
In CEF terms:
- Acceptance is primarily the intentional activation of Receptive Manifestation (Accepting), often paired with the observational function of Inquisitive Sensing (mindfulness).1
-
Values-Driven Action is the dynamic interplay between Decisive Knowing (clarity of choice) fueling Assertive Drive (Boosting) and Strategic Order (Arranging) (execution).1
By structurally defining these mechanisms, CEF moves the discourse beyond the philosophical debate between traditional Cognitive Behavioral Therapy (CBT) and ACT.19 Instead, it allows the clinician to structurally identify which specific core capacity related to acceptance or change is blocked or weak, enabling focused, skill-based interventions and the empirical validation of specific change mechanisms .
V. Mastery and Future Vision: The Path to Sustainable Affective Efficacy
The Core Emotion Framework offers a profound additive contribution to affective science by providing a robust structural-constructivist model capable of addressing psychological challenges resistant to conventional treatment.1 The framework successfully translates the goal of improving emotional granularity from a descriptive psychological measure into a prescriptive, mechanistic intervention target.5
By defining psychological distress as the pathological fusion of specific Core Emotions and the resulting breakdown of the functional hierarchy, CEF provides a high-resolution etiology for conditions such as ruminative inertia and maladaptive perfectionism. The accompanying methodology, Adaptive Emotional Cycling (AEC), offers precision protocols designed to "detangle" these fusion states by forcing structured movement between complementary Core Emotions.4 This represents a significant advancement toward individualized precision treatment.
Future translational research should focus on empirically validating the efficacy of AEC by measuring the changes in the dynamic range and speed of Core Emotion activation, utilizing advanced experience sampling methods to extend existing findings on granularity enhancement.5 Clinical tool development should leverage the CEF structural map to rapidly diagnose the specific functional short-circuit (Head, Heart, or Gut) and prescribe tailored AEC protocols based on the client's measured dominant (rigid) and deficient Core Emotions.1 Furthermore, investigating the potential of using strong Core Emotions as measured client strengths to predict success in specific AEC protocols will maximize therapeutic momentum and reinforce self-efficacy.18
This work is presented in integration with existing knowledge and models, and is particularly relevant for practitioners who have not devoted even minimal time to examining the Core Emotion Framework (CEF) in its original form. A direct engagement with the CEF’s core emotions demonstrates that the essential task lies in processing each emotion individually; through this process, the broader psychological composition takes shape in a coherent and integrated manner—regardless of the presenting issue, its origin, or whether it was ever formally diagnosed.
Works cited
- Core Emotion Framework, accessed October 20, 2025, https://www.coreemotionframework.com/
- Dimensional models of personality disorders: Challenges and opportunities - PMC, accessed October 20, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC10028270/
-
The circumplex model of affect: An integrative approach to affective neuroscience, cognitive development, and psychopathology - PubMed Central, accessed October 20, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC2367156/
- OptimizeYourCapabilities.pro, accessed October 20, 2025, https://optimizeyourcapabilities.pro/
- Rigidity (psychology) - Wikipedia, accessed October 20, 2025, https://en.wikipedia.org/wiki/Rigidity_(psychology)
- Discovering Client Strengths in Therapy Sessions (with Examples) - Blueprint, accessed October 20, 2025, https://www.blueprint.ai/blog/discovering-client-strengths-in-therapy-sessions-with-examples
- Experiential Avoidance Process Model: A Review of the Mechanism for the Generation and Maintenance of Avoidance Behavior - Psychiatry and Clinical Psychopharmacology, accessed October 20, 2025, https://psychiatry-psychopharmacology.com/en/experiential-avoidance-process-model-a-review-of-the-mechanism-for-the-generation-and-maintenance-of-avoidance-behavior-133252
- Obsessive-Compulsive Personality Disorder (OCPD): Symptoms - Cleveland Clinic, accessed October 20, 2025, https://my.clevelandclinic.org/health/diseases/24526-obsessive-compulsive-personality-disorder-ocpd
- Ruminative Inertia, Emotion Regulation, and Depression: A Daily-Diary Study, accessed October 20, 2025, https://www.researchgate.net/publication/351373643_Ruminative_Inertia_Emotion_Regulation_and_Depression_A_Daily-Diary_Study
- Cognitive Biases and the Emotional Disorders - Northwestern Scholars, accessed October 20, 2025, https://www.scholars.northwestern.edu/en/publications/cognitive-biases-and-the-emotional-disorders
- Emotion Regulation in Schema Therapy and Dialectical Behavior Therapy - Frontiers, accessed October 20, 2025, https://www.frontiersin.org/journals/psychology/articles/10.3389/fpsyg.2016.01373/full
- Experiential Avoidance Process Model: A Review of the Mechanism for the Generation and Maintenance of Avoidance Behavior - PMC - PubMed Central, accessed October 20, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC11332439/
- Despair | Research Starters - EBSCO, accessed October 20, 2025, https://www.ebsco.com/research-starters/health-and-medicine/despair
- The PERMA Model: Your Scientific Theory of Happiness - Positive Psychology, accessed October 20, 2025, https://positivepsychology.com/perma-model/
- How to do strengths-based therapy & interventions (With Examples) - Mentalyc, accessed October 20, 2025, https://www.mentalyc.com/blog/how-to-do-strengths-based-therapy-interventions
- Perfectionism and OCPD: When Standards Hurt | Houston, TX, accessed October 20, 2025, https://houstondbtcenter.com/struggling-with-ocpd-why-perfectionism-treatment-matters-for-mental-health/
- Acceptance and Commitment Therapy and Psychological Well-Being: A Narrative Review, accessed October 20, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC11837766/
- Negative rumination in depression subtypes with melancholic features and anxious distress - PMC, accessed October 20, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC11865946/
- Evaluating Acceptance and Commitment Therapy: An Analysis of a Recent Critique - ERIC, accessed October 20, 2025, https://files.eric.ed.gov/fulltext/EJ959657.pdf
- Optimizeyourcapabilities.com. (2025). The Core Emotion Framework (CEF): A Theoretical Synthesis Integrating Affective Neuroscience, Embodied Cognition, and Strategic Emotional Regulation for Optimized Functioning [Zenodo]. https://doi.org/10.5281/zenodo.17477547
- Optimizeyourcapabilities.com. (2025, November 14). A Proposal for Open Validation of the Core Emotion Framework (CEF): A Structural-Constructivist Model for Emotional Regulation and Psychological Flourishing. https://doi.org/10.17605/OSF.IO/SG3KM
- Bulgaria, J. (2025). Compendium of Evidence-Based Psychotherapy Modalities: Reframed through the Core Emotion Framework (CEF). Zenodo. https://doi.org/10.5281/zenodo.17665533
- Bulgaria, J. (2025, November 21). Pre-Registration Protocol: Open Validation of the Core Emotion Framework (CEF) Scale – Phase 1: Construct Definition, Item Generation, and Multi-Level Factor Structure Confirmation. https://doi.org/10.17605/OSF.IO/4RXUV
- Bulgaria, J. (2025). The Core Emotion Framework (CEF): A Structural-Constructivist Model for Emotional Regulation and Adaptive Resilience in the Treatment of Anxiety. Zenodo. https://doi.org/10.5281/zenodo.17693163
- Bulgaria, J. (2025). Extending the Core Emotion Framework: A Structural-Constructivist Model for Obsessive- Compulsive Disorder (OCD). Zenodo. https://doi.org/10.5281/zenodo.17713676
- Bulgaria, J. (2025). Structural Psychopathology of Major Depressive Disorder_ An Expert Validation of the Core Emotion Framework (CEF). Zenodo. https://doi.org/10.5281/zenodo.17713725