The Emotion-First Solution to Addiction: Discover CEF’s Groundbreaking Method
What if addiction wasn’t the problem—but a symptom? The Core Emotion Framework (CEF) flips conventional recovery on its head by addressing the emotional architecture beneath addictive behaviors. Addiction recovery is evolving—and emotional intelligence is leading the way.
The Core Emotion Framework (CEF) is a cutting-edge system designed to help individuals understand and rewire the emotional drivers of addiction. By integrating neuroscience, trauma-informed therapy, and emotional mapping, CEF offers a holistic path to freedom that’s both science-backed and soul-centered.
Unlocking Sobriety: How the Core Emotion Framework Reveals the Blueprint for Addiction Recovery
Discover a revolutionary approach to understanding and overcoming addiction using the Core Emotion Framework (CEF). Moving beyond traditional concepts of 'positive' and 'negative' emotions, the CEF views emotional states as a foundational 'internal operating system' composed of ten core functions. When addiction takes hold, this entire emotional architecture—including Sensing, Calculating, and Deciding—collapses, leading to the loss of control and the failure of crucial executive functions. This structural analysis provides a blueprint for leveraging next-generation emotional intelligence to restore internal stability, regain self-mastery, and design a sustainable pathway to long-term sobriety and resilience.
Addiction recovery has entered a new era with the Core Emotion Framework (CEF), a transformative approach developed by OptimizeYourCapabilities.com. Unlike traditional addiction treatment models that focus solely on behavior or substance control, CEF dives deep into the emotional roots of addiction—uncovering emotional misalignment, unresolved trauma, and subconscious patterns that fuel dependency. By leveraging emotional recalibration techniques, CEF empowers individuals to break free from addictive cycles, restore emotional balance, and build a resilient, purpose-driven life.











The Core Emotion Framework (CEF) and Addiction: A Structural Analysis of Emotional Function Collapse and Restoration

I. Introduction: Addiction as a Crisis of Emotional Function Design
Addiction, clinically defined as Substance Use Disorder (SUD), is a chronically relapsing disorder characterized by a destructive cycle of compulsion, the loss of executive control over intake, and the subsequent emergence of negative emotional states during abstinence or withdrawal.2 It manifests fundamentally as a syndrome of dysregulated motivation.3 The transition from occasional, controlled substance use to a chronic addicted state involves profound shifts in specific neurocircuits, marked by the compromise of frontal cortical areas responsible for high-level executive function and the pathological sensitization of striatal systems governing incentive motivation.2
The Core Emotion Framework (CEF) offers a groundbreaking conceptualization of human behavior, viewing emotions not as static states, but as actionable processes constituting an "internal operating system" or blueprint for emotional responses. This framework moves beyond simplistic binaries of positive and negative emotion, proposing ten distinct core emotional functions, each possessing a unique energy vital for success, connection, and meaning.1 Based on this model, addiction can be meticulously analyzed as a critical systemic failure of emotional architecture, where these ten core functions become pathologically distorted, misdirected, or hyper-sensitized toward a single, destructive object or behavior.
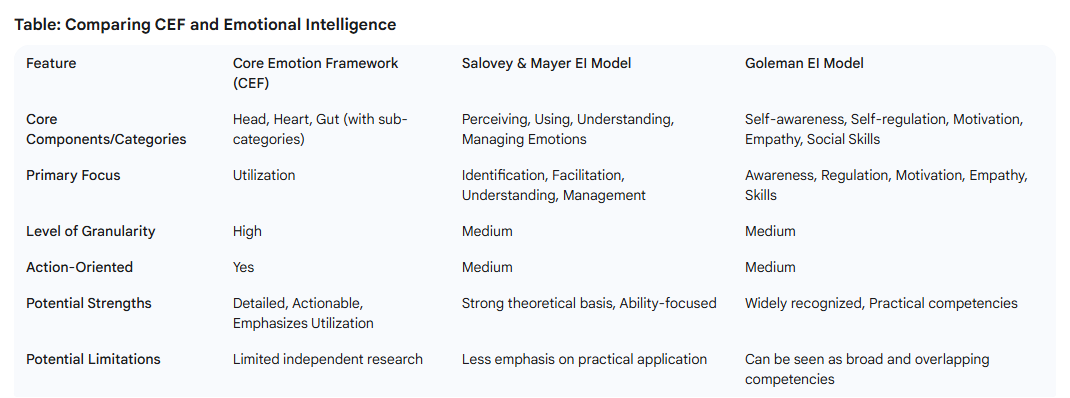
1.2. The Core Emotion Framework (CEF): A Tripartite Model of Agility
The CEF structures emotional processing into an integrated tripartite system.1 This system illuminates how emotional states directly influence rational processes, social interactions, and motivation:
- Head (Cognition & Decision-Making): Governs rational thought, analysis, and strategic choice. It encompasses the functions of Sensing, Calculating, and Deciding.
- Heart (Connection & Emotional Flow): Encompasses emotions tied to empathy, relationships, emotional resonance, and boundaries. It includes Expanding, Constricting (Precising), and Achieving (Juggling).
- Gut (Action & Motivation): Drives emotions linked to initiation, execution, sustained drive, and self-management. This sphere involves Arranging (Managing), Appreciating (Clapping), Boosting, and Accepting (Surrendering).1
This analysis applies the standanrd CEF terminology while noting the corresponding conceptual terms from some framework pages where they differ: Constricting (Precising), Achieving (Juggling), Arranging (Managing), Appreciating (Clapping), and Accepting (Surrendering).1
II. The Head Center: The Cognitive Collapse (Sensing, Calculating, Deciding)
The Head Center functions are foundational to filtering external reality, evaluating consequence, and executing control.1 The integrity of these functions is directly tied to the prefrontal cortex (PFC), which suffers significant impairment due to chronic substance abuse.5 The pathology of addiction originates, in part, from the systemic breakdown of these cognitive-emotional functions.
2.1. Sensing: The Distorted Information Stream
The emotional function of Sensing is defined as the capacity for initial perception, observation, and the gathering of raw factors, emotions, or intensities from the internal and external environment.4 It serves as the primary input mechanism of the emotional operating system.
In the addictive state, this critical sensory function is hijacked by the phenomenon of incentive salience.6 Neuroscientific research indicates that addiction distorts the systems mediating 'wanting' versus 'liking' through enduring sensitization of brain dopamine systems.6 Consequently, drug-associated cues acquire a pathological level of incentive salience; the sensory input (Sensing) related to the substance—such as the sight of paraphernalia or the memory of a setting—is dramatically amplified and prioritized by the neurochemical reward pathways.3 The individual's Sensory function ceases to provide a neutral perception of the environment. Instead, it becomes pathologically biased, filtering out irrelevant sensory input while highlighting and prioritizing cues that trigger the compulsive drive for drug-seeking behavior.
2.2. Calculating: Maladaptive Analysis and Rumination
Calculating encompasses the ability to perform in-depth analysis, logically process data, resolve puzzles, and evaluate information derived from raw sensory input.4 This function is meant to generate strategic understanding and informed choice.
In addiction, the energy of Calculating is severely misdirected, resulting in non-constructive rumination. Instead of engaging in objective analysis or constructive problem-solving, the individual's cognitive resources are monopolized by repetitive, circular dwelling on negative feelings, personal distress, and the perceived causes and consequences of their problems. This negative cognitive loop makes it extraordinarily difficult to move toward practical solutions or analyze situations objectively.7
Furthermore, chronic drug use compromises the structural function of the prefrontal cortex, which is essential for rational risk assessment and the evaluation of long-term consequences. The Calculating function, crucial for objectively weighing immediate gratification against long-term well-being, fails, leading to distorted priorities.5
The fundamental collapse of the decision-making process is initiated by a cascade involving these two functions. The neurological sensitization of the 'Sensing' function leads to a pathological hyper-activation of drug cues. This overwhelming sensory input subsequently impairs the 'Calculating' function, rendering objective risk assessment and rational analysis ineffective because the emotional and chemical pull of the craving outweighs rational consideration. This establishes a structural failure in information processing and evaluation that precedes the choice itself.
2.3. Deciding: The Failure of Inhibitory Control and Prioritization
Deciding represents the power to make definitive choices, commit to a path, and resolve ambiguities by achieving clarity based on the interaction of logic and emotion, thus setting priorities.4
The signature characteristic of all addictive disorders is the profound loss of control over one's behavior.10 The Deciding function fails because the neurocircuits responsible for behavioral execution and inhibitory control are severely compromised.2 Addiction is conceptualized as progressing through stages, shifting from impulsive drug use (driven by the initial positive rush) toward compulsive use (driven by the avoidance of negative emotional states, or withdrawal). Impaired inhibitory control—the inability to say "no"—is central to the failure of Deciding, massively increasing the probability of drug-seeking behaviors even in the face of negative consequences.10
While an individual may rationally understand the destructive nature of their behavior (a potential success of Calculation) and truly desire abstinence, the ability to execute and commit to that choice (Deciding) is derailed by neuroadaptive changes in the PFC and ventral striatum. The Deciding function, therefore, loses its ability to prioritize long-term goals over immediate, chemically enforced urges. Complementing this, when the Calculating function becomes locked in non-constructive rumination, it generates a persistent negative affective state.7 This cognitive loop feeds the reliance on substances for emotional avoidance, thereby intensifying the negative reinforcement cycle that the failed Deciding function cannot overcome, leading to chronic failures of self-control.
III. The Heart Center: Emotional Dysregulation, Connection, and Execution (Expanding, Constricting, Achieving)
The Heart Center governs affective processes, including connection, openness, and boundaries, and, in this configuration, goal execution.1 Addiction pathology in this center is marked by pervasive emotional dysregulation, the inability to manage feeling states, and a detachment from the natural emotional and social environment.
3.1. Expanding: The Contraction of Self and Worldview
Expanding is the emotional drive for openness, connection, curiosity, and embracing new experiences.1 It is the mechanism that allows for growth, social bonding, and the discovery of meaning beyond immediate survival needs.
In the context of addiction, the drive for Expanding undergoes severe contraction. Chronic substance use results in the emotional system biasing processing toward drug-related cues, simultaneously devaluing and neglecting natural rewards—such as fulfilling relationships, hobbies, or professional growth.12 The vast emotional and experiential landscape that Expanding seeks becomes severely narrowed, focusing almost exclusively on the substance and its associated pursuit. This psychological narrowing contributes significantly to social isolation and the inability to find joy or meaning in non-drug activities, which in turn deepens the vulnerability to negative affect states and reinforces compulsive consumption.12
3.2. Constricting (Precising): Boundary Failure and Emotional Dysregulation
Constricting (Precising) involves the emotional need for clarity, establishing boundaries, refining details, and achieving accuracy.1 It is the emotional function underpinning self-control and the regulation of internal and external borders.
The deficit in Constricting (Precising) is critical. Physiologically, it manifests as impaired inhibitory control.10 Psychologically, it results in severe emotional dysregulation and profound difficulties with establishing personal boundaries.13 Emotional dysregulation—the inability to effectively experience, process, or manage overwhelming emotions—drives individuals toward maladaptive coping mechanisms, most notably substance use, to numb or control distressing internal feelings.14
The failure of Constricting is further complicated by its maladaptive application. Individuals with SUDs frequently exhibit a greater reliance on expressive emotional suppression.17
Suppression is an inflexible, rigid attempt to apply the Constricting function to limit the outward expression of emotion, often in social contexts to maintain a false appearance of stability.6 However, this rigid suppression proves counterproductive, fueling underlying emotional instability, heightening stress14, and failing to solve the root problem of overwhelming internal affect. This failure to constructively regulate internal boundaries means the individual is perpetually reliant on external agents (the substance) to manage affective flux.
Crucially, the failure of Constricting drives the contraction of Expanding. When maladaptive Constricting is employed as rigid suppression, the individual cannot effectively regulate or tolerate uncontrolled negative emotions. Consequently, they must limit their sphere of life experience (Contracting - Expanding) because genuine openness, curiosity, or connection would expose them to overwhelming, painful feelings that they lack the capacity to process or regulate effectively through healthy Constricting. This explains why emotional avoidance becomes central to maintaining the addictive structure.
3.3. Achieving: Misdirected Drive and Self-Sabotage
Achieving represents the energy for action, execution, multi-tasking, and successfully attaining goals.1 It is the driving force behind effective performance.
In the addiction syndrome, the energy of Achieving is profoundly diverted and misdirected. Behavior shifts from being goal-oriented (purposeful pursuit of a desired outcome) to strictly habit-based (automatic, inflexible responding to internal and external cues).3 The Achieving function, once aimed at constructive life goals, is captured by the compulsive pursuit of the substance, creating a system where the attainment of the substance becomes the primary—and often the only—successful execution.
When this pathologically redirected Achieving energy interferes with critical, long-standing personal objectives (such as career, family stability, or financial health), it is recognized clinically as self-sabotage. The individual engages in compulsive behaviors, such as substance abuse or procrastination, that actively undermine their stated long-term success, effectively setting up roadblocks on their own path. The inclusion of Achieving in the Heart Center reflects how the failure to execute healthy goals is tied to the emotional core's loss of integrity, channeling energy toward the substance rather than human connection and growth.
IV. The Gut Center: Action, Motivation, and Structural Stability (Arranging, Appreciating, Boosting, Accepting)
The Gut Center dictates motivational drive, organization, and behavioral stability.1 The pathology here reflects the translation of cognitive and affective dysregulation into manifest behavioral loss of control, particularly in structuring a sober life.
4.1. Arranging (Managing): Impaired Organization and Prioritization Deficits
Arranging (Managing) is defined as the ability to organize, lead, coordinate, and ensure stability and control.1 This function provides the structural framework of executive control essential for daily life.
Substance addiction severely impairs executive function, which is intrinsically tied to the Arranging capacity. This impairment, localized in the prefrontal cortex, includes a diminished ability to organize thoughts and activities, prioritize tasks, manage time, and regulate impulses.19 The collapse of this function means the addicted individual struggles to maintain the structure, planning, and strategic oversight required for abstinence and recovery. The failure of Arranging in the Gut Center means the individual lacks the internal capacity to order their life and environment, leading to the behavioral chaos that reinforces reliance on external agents for control. If this organizing function is impaired, sustained goal pursuit is inherently undermined.
4.2. Appreciating (Clapping): Anhedonia and the Devaluation of Life
Appreciating (Clapping) is the emotion associated with joy, recognition, celebration, and acknowledging success, both internal and external.1 It is essential for providing positive internal reinforcement for healthy behavior.
Addiction introduces a state of pervasive anhedonia—the reduced capacity to experience pleasure—and generalized reward hypo-sensitivity.12 While the brain's reward system becomes hyper-sensitized specifically to the pharmacological effects of the drug (Sensitization), it loses the capacity to register, value, or celebrate natural, non-drug-related accomplishments or pleasures.7 This severe deficit in Appreciating, residing in the Gut Center's motivational sphere, ensures that any significant non-drug success (e.g., repairing relationships, achieving sobriety milestones) fails to generate the necessary motivational currency to sustain recovery.3 The absence of endogenous reward mechanisms for healthy behavior reinforces the bias toward the artificially potent reward of the drug.
This affective pathology forms a destructive feedback loop in the Gut Center. The deficit in Appreciating (anhedonia) guarantees a perpetually negative emotional baseline (dysphoria or negative affect).2 This dysphoric state directly necessitates the use of substances for mood management, which, in turn, sustains dependency by removing the internal reward for sobriety.
4.3. Boosting: The Exhaustion of Motivational Reserve
Boosting is the desire to inspire, motivate, uplift, and empower oneself and others.1 It is the generator of internal drive and self-efficacy.
Chronic drug use systematically exhausts or externalizes the natural motivational reserve. The substance itself provides an artificial, chemically induced "boost," effectively replacing the natural functioning of the motivation circuits.14 Research utilizing fMRI has demonstrated abnormal functioning in the midbrain—a key region governing motivation—in addicted individuals, particularly when faced with demands for sustained effort or inhibitory control.21 The system becomes dependent on external chemical stimuli, making internal, self-generated motivation increasingly difficult to access or sustain. Therefore, therapeutic modalities focused on recovery, such as Motivational Interviewing, must specifically target and enhance the client's intrinsic, internal motivation (restoring Boosting) to ensure sustained behavior change, recognizing that extrinsic motivation or fear-based approaches are insufficient.12
4.4. Accepting (Surrendering): The Overcoming of Learned Helplessness
Accepting (Surrendering) is the core emotional capacity for adaptability, letting go of rigid control, and flowing constructively with circumstances.1 It relates to resilience and emotional endurance.
In the addictive state, the failure of Accepting is dual: first, as previously noted, it involves emotional avoidance, where substances are used to escape or fail to constructively process distressing internal feelings.14 Second, and more critically, it manifests as Learned Helplessness.19 Due to repeated, failed attempts to control substance use or overcome overwhelming life problems, the individual develops the cognitive belief that "nothing I do will make any difference". This learned helplessness represents a passive resignation to their circumstances, leading them to stop trying to change even when the capability for change exists.19 Feelings of hopelessness and helplessness are documented to rapidly trigger relapse.21
The functionality of Accepting is a prerequisite for the restoration of Boosting. If an individual is entrenched in learned helplessness (pathological failure of Accepting), external efforts to enhance motivation (Boosting) are unlikely to succeed.16 Recovery requires teaching the constructive power of Acceptance—not passive resignation, but the radical acknowledgment of reality—as the essential step for overcoming learned helplessness. By cultivating a positive internal dialogue and learning to constructively explain events, therapeutic interventions can break the cycle of powerlessness and enable the individual to access and utilize their intrinsic motivational energy (Boosting).19
V. Synthesis: Rebuilding Emotional Fluency for Recovery
5.1. The Interplay of Pathology: From Impulsivity to Systemic Failure
Addiction is marked by a clear progression: a shift from impulsive behavior, which is primarily a failure of the Head Center (Deciding, Constricting) related to positive reinforcement, toward compulsive behavior, which is a habit-based failure of the Gut Center (Arranging, Appreciating) maintained by negative reinforcement and withdrawal avoidance. This progression signifies a systemic collapse of the emotional operating system where the rational processing network (Head) is overwhelmed and hijacked by the pathologically sensitized motivational and habit centers (Gut), a process powerfully mediated and maintained by affective dysregulation (Heart).
The CEF provides a practical diagnostic blueprint for assessing the specific functional deficit. The question is not simply "Why does the person use?" but rather, "Which core emotional function is failing?" Is the primary issue hyper-sensitized Sensing (cue hypersensitivity), resulting in an overwhelming urge? Is it impaired Arranging (organizational collapse), preventing structured sobriety? Or is it a failure of constructive Accepting (learned helplessness), leading to passive resignation?
Therapeutic efforts focusing solely on strengthening Deciding (inhibitory control) will prove insufficient if the Sensing input remains pathologically overwhelming or the Accepting function remains resigned to failure. Effective treatment must target the appropriate centers sequentially or simultaneously.
5.2. Therapeutic Reconstitution: Mastering the Ten Functions
The framework emphasizes moving beyond mere emotional awareness to the intentional, actionable application of emotional energy.1 Recovery is the process of learning to consciously engage beneficial functions and skillfully disengage detrimental ones.
Restoration of executive function requires intensive work on strengthening inhibitory control (Deciding and Constricting)10 and implementing cognitive behavioral strategies to halt negative thinking patterns (Calculating).7 Sustained sobriety necessitates the intentional redirection of attention away from drug cues (recalibrating Sensing) and the active cultivation of appreciation for life's non-drug rewards (Appreciating).12 Furthermore, the individual must intentionally foster curiosity and embrace complexity (Expanding) to counteract the affective narrowing induced by addiction.
The ultimate goal of this reconstitution is the mastery of Emotional Fluency.1 This state represents the ability to rapidly shift between and articulate various emotional states, providing profound internal resilience. This agility is fundamentally dependent on the functional restoration of constructive
Accepting (Surrendering), which allows the individual to navigate distress without resorting to maladaptive coping mechanisms like suppression or substance use.14 By cultivating an intentional, constructive relationship with all ten core emotional energies, the individual can transition from an externally controlled, pathologically driven state to one of intentional impact and self-mastery.1
VI. Conclusion: Emotional Architecture and Long-Term Resilience
Drug addiction represents a profound architectural failure of the human emotional operating system, leading to cognitive impairment and affective dysregulation rooted in neurobiological sensitization and frontal lobe compromise. The Core Emotion Framework provides a detailed vocabulary and a precise blueprint for understanding this systemic failure by mapping pathology across the Head, Heart, and Gut Centers.
The pathway to enduring recovery involves the meticulous, center-by-center restoration of these core functions. This restorative process demands not only the strengthening of inhibitory control (Deciding/Constricting) and organizational capacity (Arranging/Managing) but also the profound re-sensitization of the reward system to natural life experiences (Appreciating/Clapping) and the leveraging of radical acceptance (Accepting/Surrendering) to overcome the pervasive psychological barrier of learned helplessness.
By recognizing emotions as powerful, actionable energies that can be designed and intentionally applied, the CEF shifts the therapeutic focus from reactive emotional management to proactive emotional system design, unlocking the necessary resilience, ethical decision-making, and intrinsic creativity (Expanding) that define long-term emotional agility and sustained well-being.1 The reconstitution of a robust emotional architecture is paramount for achieving tangible success and enduring recovery in an interconnected, complex world.
Works cited
- Optimize Your Capabilities | Everything is Already Inside There, accessed September 28, 2025, https://optimizeyourcapabilities.com
- Neurobiology of Addiction | Focus - Psychiatry Online, accessed September 28, 2025, https://psychiatryonline.org/doi/10.1176/foc.9.1.foc55
-
Motivational Processes Underlying Substance Abuse Disorder - PMC - PubMed Central, accessed September 28, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC4851611/
- OptimizeYourCapabilities.pro, accessed September 28, 2025, https://optimizeyourcapabilities.pro
- Addiction And The Brain: How Drugs Impact The Brain - Conifer Park, accessed September 28, 2025, https://www.coniferpark.com/blog/addiction-and-the-brain
- Liking, Wanting and the Incentive-Sensitization Theory of Addiction - PMC - PubMed Central, accessed September 28, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC5171207/
- Rumination: A Cycle of Negative Thinking - American Psychiatric Association, accessed September 28, 2025, https://www.psychiatry.org/news-room/apa-blogs/rumination-a-cycle-of-negative-thinking
- Self-Sabotage | Psychology Today, accessed September 28, 2025, https://www.psychologytoday.com/us/basics/self-sabotage
- How Addiction Impacts Decision-Making Abilities - Samba Recovery, accessed September 28, 2025, https://www.sambarecovery.com/rehab-blog/how-addiction-impacts-decision-making-abilities
- Response inhibition and addiction medicine: From use to abstinence - ResearchGate, accessed September 28, 2025, https://www.researchgate.net/publication/310842596_Response_inhibition_and_addiction_medicine_From_use_to_abstinence
- Learned Helplessness | Psychology Today, accessed September 28, 2025, https://www.psychologytoday.com/us/basics/learned-helplessness
- The detrimental effects of emotional process dysregulation on decision-making in substance dependence - PubMed Central, accessed September 28, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC3491319/
- Addiction and autonomy: Why emotional dysregulation in addiction impairs autonomy and why it matters - Frontiers, accessed September 28, 2025, https://www.frontiersin.org/journals/psychology/articles/10.3389/fpsyg.2023.1081810/full
- The Link Between Emotional Suppression and Substance Abuse, accessed September 28, 2025, https://www.newhorizonscenters.com/blog/the-link-between-emotional-suppression-and-substance-abuse
- Why Do We Self-Sabotage? The Psychology Behind Destructive Habits, accessed September 28, 2025, https://insightspsychology.org/self-sabotage-psychology-destructive-habits/
- Chapter 1—A New Look at Motivation - Enhancing Motivation for Change in Substance Use Disorder Treatment - NCBI, accessed September 28, 2025, https://www.ncbi.nlm.nih.gov/books/NBK571073/
- Emotion regulation in substance use disorders: a systematic review and meta‐analysis, accessed September 28, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC10087816/
- Capturing naturally occurring emotional suppression as it unfolds in couple interactions, accessed September 28, 2025, https://repository.brynmawr.edu/cgi/viewcontent.cgi?article=1065&context=psych_pubs
- THE NEUROBIOLOGY OF SUBSTANCE USE, MISUSE, AND ADDICTION - NCBI, accessed September 28, 2025, https://www.ncbi.nlm.nih.gov/books/NBK424849/
- MOTIVATION FOR CHANGE: OVERCOMING HELPLESSNESS, accessed September 28, 2025, https://files-profile.medicine.yale.edu/documents/ff6f5c75-7b5f-4236-9af5-9dc3605225ce
- Mental Fatigue Impairs Brain Function, Motivation in Drug-Addicted Individuals | BNL Newsroom - Brookhaven National Laboratory, accessed September 28, 2025, https://www.bnl.gov/newsroom/news.php?a=111465
- Optimizeyourcapabilities.com. (2025). The Core Emotion Framework (CEF): A Theoretical Synthesis Integrating Affective Neuroscience, Embodied Cognition, and Strategic Emotional Regulation for Optimized Functioning [Zenodo]. https://doi.org/10.5281/zenodo.17477547
- Optimizeyourcapabilities.com. (2025, November 14). A Proposal for Open Validation of the Core Emotion Framework (CEF): A Structural-Constructivist Model for Emotional Regulation and Psychological Flourishing. https://doi.org/10.17605/OSF.IO/SG3KM
- Bulgaria, J. (2025). Compendium of Evidence-Based Psychotherapy Modalities: Reframed through the Core Emotion Framework (CEF). Zenodo. https://doi.org/10.5281/zenodo.17665533
- Bulgaria, J. (2025, November 21). Pre-Registration Protocol: Open Validation of the Core Emotion Framework (CEF) Scale – Phase 1: Construct Definition, Item Generation, and Multi-Level Factor Structure Confirmation. https://doi.org/10.17605/OSF.IO/4RXUV